
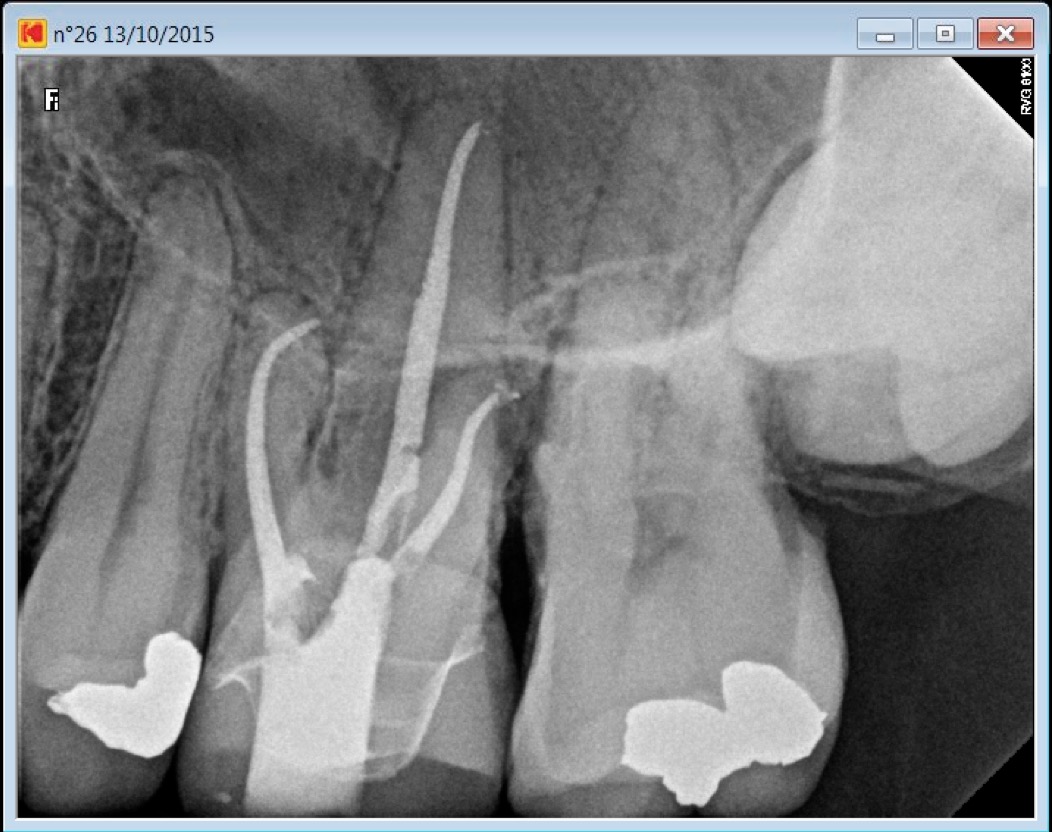

Patient came in on an emergency basis presenting with pain and a swollen left cheek. Access cavity through existing crown, pulp stones removal, four canal entries location, complete shaping and cleaning of three canals out four have been completed during the first setting. Also allowed 30 minutes for drainage, lots of irrigation (Sodium hypochlorite 6%), interim Calcium Hydroxide dressing. MB2 root canal entry has been located with the help of a Zeiss dental operating microscope and a Buc 3 ultrasonic tips (Spartan). Due to a lack of time, we had to make the patient come back for the second mesiovestibular root canal procedure, patient has also been given a course of antibiotics.
The fourth canal took an extra hour to perform. Root canal shaping performed with Mani K files, Pro Taper Universal and landed files, obturation technique was warm vertical condensation and Pulp Canal Sealer. Composite core build up.
Hello chief.
Great case.
I have two questions for you.
First is second radio the obturation With hydroxyde of calcium. ? It is very dense. I m notre used seeing this density with calcium s hydroxyde.
Second you talk about an hour to manage to treat mv2 canal. Was the canal totally obliterated?or calcified?
I m usually confronted to this Kind of situations. I begin to open the entry of thé canal with us spartan with my kaps microscope. And I try to follow the color of calcification. But often I Wonder if I have to continue with us or not? You see my question. You tell you used many k files. ?you Just used them to find patency of the canal or you altern with us?
Congratulations for this case.it s very interesting
Thank you Doc,
I use Metapex Calcium hydroxide with iodophorm, I think it contains a lot of Barium sulfate which is the radio opacifier responsible for this density you are seing on the post operative Xray.
Yes it took an hour to shape the MB2 because it was completely calcified. In fact you are wright when you say I alternate, first I locate the canal entry than I try with a K file and if I do not have patency than I keep on using US, then I try again … and so on until I obtain the canal patency
Hope this could be of some help
thank you for your response.
you gave me some important indications.
can you precise me how do you do to put metapex into the root. DO you use lentulo? or some stuff like that.
other thing: i guess you use warm vertical condensation.What system do you use? i’m using mac spadden technique but i would change and use WVC. I just tested some of systems, like calamus (dentsply) and sybron but my choice isn’t arrested.
What could you advice me please?
Thank you and have a nice day
You do not need a paste filler to insert Metapex Calcium Hydroxide into the canal, the syringe comes with long and narrow disposable plastic tips. Sometimes those plastic tips are sealed at their extremity due to to a manufacturing issue, in that case you can cut one mm off from the tip with a number 15 surgical blade , et voilà! There is a twist though in order not to overfill with calcium Hydroxide, I usually extrude a little bit of the paste outside of the patient’s mouth in order to evaluate the pressure I have to exert to obtain the right amount. Then I bring the tip as close as possible to the apex and I redraw it for about 1 mm or two before applying a slight pressure. You need to apply this pressure while you are slowly redrawing the tip from the canal. Some training on used transparent endo acrylic blocs may be useful to get the feeling of it in your own hands. If you do extrude Calcium Hydroxide do not worry too much as it is NOT an issue as so many of us have been taught. For my backfill in WVC I have been using the Obtura System from Spartan Company for the last 20 years (roughly). I am probably still using it because I got used to it and thus I feel I have more control on my backfill, also because they probably were the first to come out with this idea and I am both grateful and faithful to them for that.
Thank you again for the response. I m very attentive to détails.
I m un fact actually doing a postgraduate in France in endodontics but honnestly I m desappointed about lac k of good materials. An old kaps very few performant, some old niti systems used which can break in an root…
I want to be really a good pratician,that s why I ll try to integrate a post graduate in Canada or in usa… so my technical questions. I really appreciate time you take to answer me with all these précisions. Thank you so much