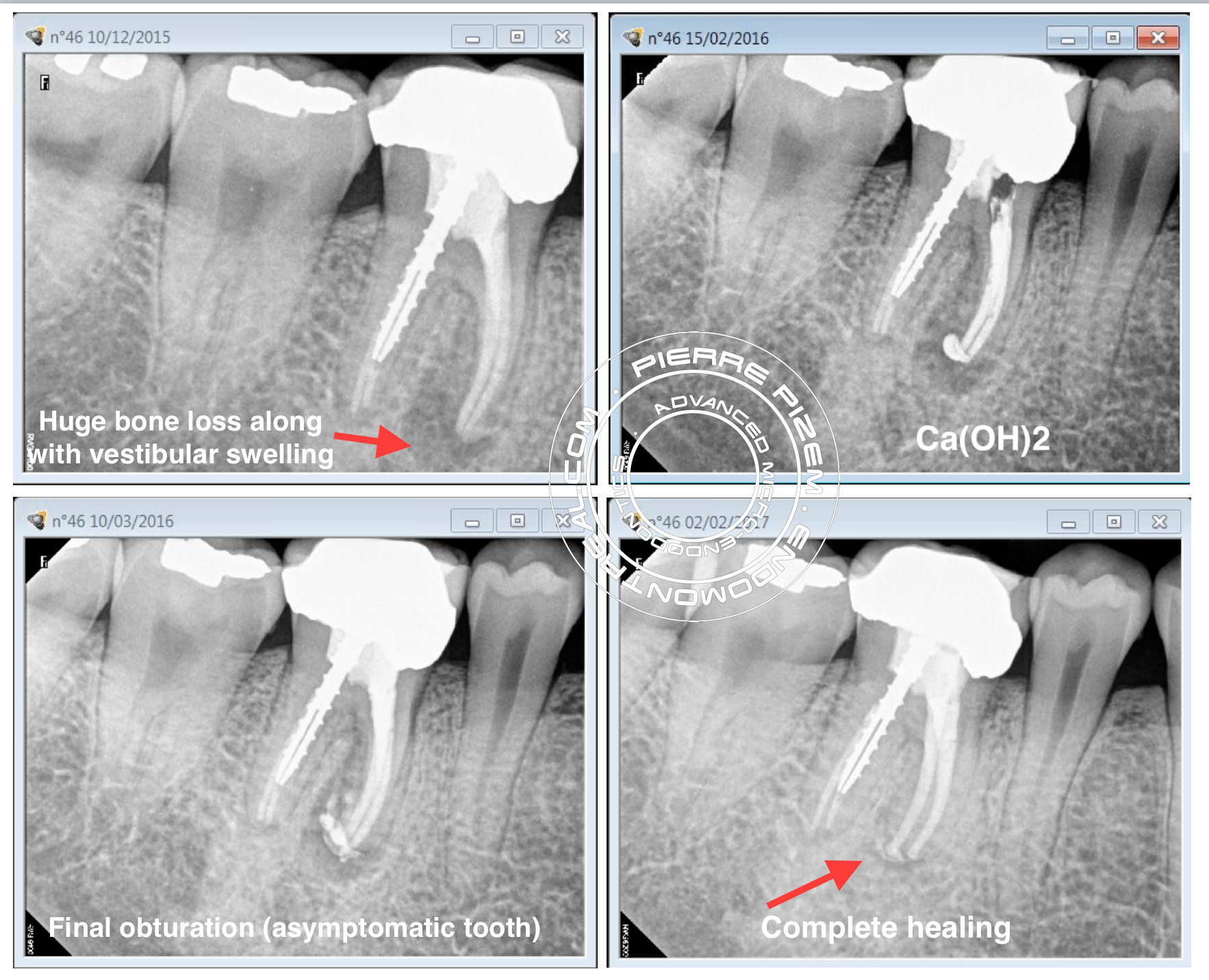
Patient came to us for a second opinion because he was previously offered to remove his lower right molar and replace it by an implant supported crown. Huge vestibular swelling and the ”J” Shape radiolucency on mesial root were the main reason why the patient was told this tooth should be extracted (”J” Shape lesions such as this one have been traditionally associated with a cracked root). Upon clinical examination swelling was gone (patient had been taking a course of antibiotics) and there was no deep and narrow pocket when probing. Thus, I offered the patient to treat his tooth with a selective root canal retreatment.
According to Nudera ”it is not always necessary that all restorative and obturation materials be removed from all roots regardless of the presence or absence of periapical pathosis” and ”Selective root canal retreatment represent a conservative treatment alternative for previously endodontically treated teeth with multiple roots presenting with post-treatment disease”. I have been successfully doing this for for the last 10 years now, and it always did lead to a successful outcome.
Procedure and armamentarium: ProTaper Universal up to size F4, NaOCl 5%, PUI for 5mn, Interim Ca(H)2, Pulp Canal Sealer, Warm Vertical Condensation.
After one year post operative X Ray image shows a complete healing. In this case the ”J” shape lesion was obvious but there were no fractures found, thus ”J” shape lesion could easily mislead a practitioner into wrongly extracting a tooth.
.
Leave a Reply