Case Study Number 456147
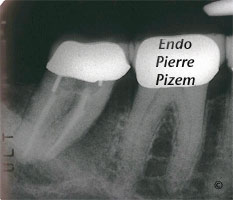
We have been presented with this mandibular second molar that has a periapical lucency which also has a periodontal component. Patient is experiencing pain. This radiographic image also shows a huge radiographic J-shaped lesion that may be indicative of a vertical root fracture in the mesial aspect of the mesial root.
Are we dealing with a periodontal infection? And, if this is the case, such a periradicular tissues loss would command an extraction of the tooth.
Are we dealing with a fracture? And, if this is the case, tooth extraction would also be the treatment of choice.
Are we dealing with an endodontic infection? If this is the case an endodontic revision (endodontic retreatment) would suffice to preserve this tooth.
The decision of extracting or saving that tooth should be based on a foundation of sound diagnosis.
One of the primary fact that needs to be established in distinguishing endo/perio lesion is the pulp status. Since there is not much pulp left in that case, pulp testing won’t help much.
Periodontal probing is the next important measurement in determining if wether this tooth has an endodontic or periodontic infection. Probing shows no wide or narrow pocket on buccal neither on lingual (and on distal) aspects of this tooth, at this stage, periodontal infection might be ruled out.
The remaining question is: “Are we dealing with a fracture or an endodontic infection?”
A deep narrow periodontal pocket would indicate a vertical root fracture and the quiz would end right there. The tooth would have to be extracted.The problem is that this defect, if it does exist, might be located just beneath a wide and tight mesial contact point and probing with accuracy this area is not that obvious. Hence the final question cannot be answered without any doubt by probing alone.
One option would be to remove the crown to allow for a direct access to the potential defect. But then, if no deep narrow periodontal pocket exist, the clamp for the rubber dam as well as tooth protection from vertical forces would require a provisional crown to be installed. Even so, probing a deep narrow periodontal pocket is not an absolute waranty that this defect is in deed a crack. It might also be a desmodontal sinus tract. Hence,drilling through the existing crown to access mesials root canals and a direct observation under magnifying lenses of a microscope seemed to be the appropriate way of confirming the presence or absence of a vertical root fracture. (But, then again if crack would have been located in the apical third of root canal system, microscope lenses would not have been of much help either…)
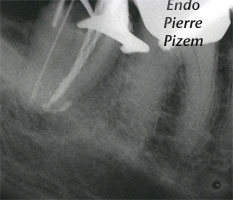

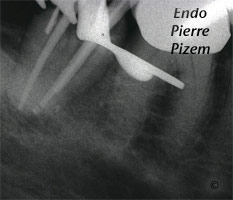

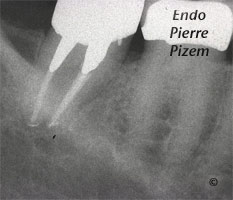
No crack could be observed from within the mesial root canals, the treatment has been completed in two appointments (third, fourth and fifth images) . Following the first appointment which implied material retrieval, irrigation and calcium hydroxyde insertion (Second X ray image), both pain and swelling disappeared. Following Xray image shows a complete periodontal tissue regeneration after one year. Tooth is asymptomatic.
Leave a Reply